

Here’s the pitch you’ll hear on half the wellness pages selling these things: LL-37, glutathione, thymosin alpha-1, they’re not foreign chemicals, they’re molecules your own body already makes. So injecting a manufactured version is basically just topping up what nature intended. Gentle. Safe. Natural.
I don’t buy it, and after going through the actual trial data and the FDA’s own paperwork, I don’t think you should either. Not because these peptides are all garbage, some of them genuinely aren’t, but because “my body makes this” and “a vial from an unverified seller is safe to inject” are two completely separate claims that the marketing quietly welds together. Let’s pull them apart.
My honest read: two different problems get mixed into one
Every time I dig into a peptide review, I try to separate the risk into two piles, because lumping them together is exactly how people talk themselves into bad decisions.
Pile one: the molecule itself, even in a perfectly pure, correctly dosed form, might do something you didn’t sign up for. Pile two: everything happening around the molecule, who made it, how clean it is, whether the vial even contains what the label claims.
Most buyers only worry about pile one, and honestly not very hard. Pile two is where the actual documented damage in this category lives. I’ll walk through both, and I’ll flag which peptides come out looking fine and which ones I’d leave on the shelf.
LL-37: the “it’s natural” argument, tested and found wanting
If you want the clearest case that “your body makes it” says nothing about safety, LL-37 is it. Reviews of the cathelicidin family describe toxicity to host cells at higher concentrations, instability in the peptide itself, and here’s the part that should stop you cold: LL-37 can act as an autoantigen, tied to autoimmune conditions including psoriasis and lupus [1]. That is your immune system learning to treat your own peptide as a threat. Not exactly the “gentle booster” billing.
There’s also early lab and animal work suggesting LL-37 might help melanoma cells and their associated macrophages invade locally [2]. I want to be fair here, that’s preclinical, not a proven human risk, and I’m not going to inflate it into something it isn’t. But it’s a real signal, and it tells me this molecule cuts both ways even when it’s pure. No large human trial has tested LL-37 at scale the way some other peptides here have been tested. That absence isn’t reassuring. It just means nobody’s looked hard enough yet to find out.
Thymosin alpha-1: solid on safety, weaker than advertised on results
This is the one compound in the lineup I’d actually call well-behaved. It’s the best-studied peptide here, generally well tolerated, with injection-site reactions as the main complaint in its track record [6]. If you’re grading purely on “does this thing hurt people,” it holds up fine.
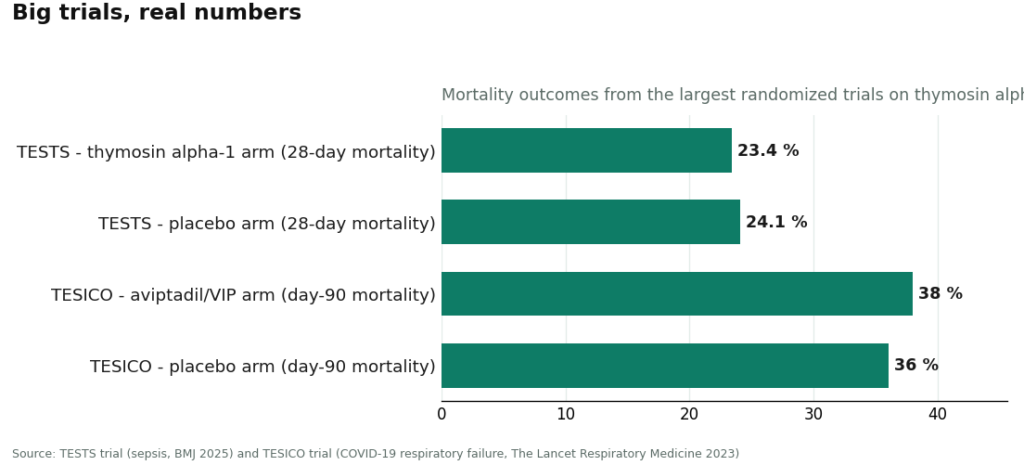
Where it stumbles is the promise, not the danger. The largest, most rigorous test of thymosin alpha-1 to date, the TESTS trial, ran 1,089 adults with sepsis and found 28-day mortality of 23.4% on thymosin versus 24.1% on placebo, a hazard ratio of 0.99 [7]. That’s not a benefit. That’s a coin flip dressed up as a trial result. So my honest read: it’s safe enough, but if you’re taking it expecting the effect the smaller, earlier studies implied, the biggest and best trial says don’t hold your breath.
VIP: nice biology, stopped for futility
VIP (tested as aviptadil) has the kind of anti-inflammatory mechanism that reads well on paper. Then it met the TESICO trial, a randomized, placebo-controlled test in COVID-19 respiratory failure, and it was stopped for futility. Day-90 mortality came in at 38% on aviptadil versus 36% on placebo [8]. Worse than placebo, not better, and the trial ended early because continuing wasn’t going to change that story.
I’m putting this next to thymosin alpha-1 on purpose, because there’s a pattern worth naming that the marketing never mentions: the peptides that actually got tested at real scale, thymosin alpha-1 and VIP, both came up short in their biggest trials. LL-37, the one with the scariest biology, hasn’t had that kind of large trial run against it at all. An untested compound isn’t a safer compound. It’s just one where the bad news hasn’t landed yet.
Glutathione: this is the case that should actually worry you
If pile-one risk is about the molecule surprising you, pile-two risk is about the supply chain betraying you, and glutathione is the textbook example. The FDA warned compounders not to use a dietary-grade glutathione powder to make sterile injectable drugs. They issued that warning after real patients had adverse events and lab tests confirmed excessive endotoxin in the product [3].
Sit with that for a second. Glutathione is the antioxidant your own cells make constantly. The molecule wasn’t the problem. The grade of the raw powder and the way it got compounded were the problem. Endotoxin doesn’t announce itself, you can’t taste it or smell it, and it can put someone in real trouble. This is the whole “natural equals safe” myth getting demolished by an actual FDA warning letter, not a hypothetical.
A vial from a research-chemical seller gives you zero visibility into raw-material grade, sterility, or endotoxin load, and there’s no licensed pharmacy standing behind it if something goes sideways. Purity and sterility aren’t features of the molecule. They’re features of the manufacturing, full stop.
There’s a quieter, less dramatic version of this same “does it even work” question with oral glutathione. Taken by mouth in its plain form, it barely reaches your bloodstream, because your gut and liver break it down before it can do anything [4]. Liposomal versions performed better in small studies [5], but I’ll flag “small studies” honestly, that’s promising, not proven. Either way, part of an honest safety review is telling you when a product might just be an expensive way to produce very dilute urine.
Thymulin: the footnote nobody puts on the label
Quick one worth knowing: thymulin’s activity depends entirely on bound zinc. In age-related thymus decline, the zinc-bound active form is basically absent, and adding zinc in vitro brings it back [9]. Translation: for some people, the real fix here might be a zinc problem, not a “let’s inject a peptide” problem. Worth asking about before you reach for the vial.
Where it actually holds up
None of this means the whole category is a bust. It means the risk split into two very different problems, and they need two very different fixes.
For the molecule-level risk, you want a clinician who can look at your actual history and say, “LL-37’s autoimmune associations make this a bad fit for you specifically” [1], or “here’s what the TESTS trial actually showed, temper your expectations accordingly” [7]. A product page can’t do that for you. No amount of reading reviews online replaces someone who knows your chart.
For the sourcing risk, the fix is boring and structural: a real, licensed pharmacy compounding under recognized standards. That’s the direct answer to the endotoxin problem the FDA documented, not a vague promise of quality, an actual accountable process [3].
This is where I land on the supervised-access model, and I’ll say it plainly since I went in skeptical: it’s the only setup here that addresses both buckets at once. FormBlends is the one I’d point to as an example worth knowing about, not because I’m selling anything (there’s nothing to buy on this page, no checkout, no affiliate link), but because a licensed physician reviewing your profile handles the molecule-fit question, and compounding through licensed 503A pharmacies under recognized standards handles the contamination question. That said, the disclosure applies here same as anywhere: compounded medications aren’t FDA-approved finished drug products, and the FDA doesn’t review them for safety, effectiveness, or quality before they hit the market [10].
The verdict
If I’m grading this category like I’d grade any product I actually tried and researched: thymosin alpha-1 gets decent marks for tolerability but a shrug for efficacy against the toughest trial data. VIP gets a pass, it looked promising and the big trial said no. LL-37 gets a hard caution, real biology, real autoimmune signal, and no big trial yet to tell us how worried to be. And injectable glutathione gets the clearest red flag in the whole bunch, not because of the molecule, but because of a documented FDA warning after real patients got hurt from a contaminated product.
The one-line summary I’d give a friend asking about this stuff: “natural” was never the safety feature here. Oversight is. Who made it, how it was tested, and whether a clinician is actually looking at your specific situation matters more than whether the molecule has a cousin already living in your bloodstream.
Questions that come up a lot
Does “my body already makes this” mean it’s safe to inject? No, and this is the myth that trips people up most. Your body makes these molecules in tightly controlled amounts, in the right place, at the right time. A vial delivers a fixed dose someone else picked, made to a standard you can’t verify. The clearest proof: injectable glutathione, something your body produces constantly, caused real patient harm once contamination entered the picture. Being “natural” didn’t protect anyone.
What’s the biggest actual risk in this category? It’s not the molecule, it’s the sourcing. The FDA’s warning against a dietary-grade glutathione powder used in sterile injectables, issued after adverse events and lab-confirmed endotoxin, is the clearest documented harm here. Endotoxin doesn’t show up on a smell test, and a research-chemical vial gives you no way to check raw-material grade or sterility.
Is LL-37 risky even in a pure form? Yes. Reviews describe toxicity to host cells at higher concentrations, instability, and LL-37 acting as an autoantigen tied to autoimmune conditions like psoriasis and lupus. There’s also early lab/animal work suggesting it might help melanoma invade locally, which is preclinical, not proven in humans, but it’s a real signal that this molecule has teeth even when it’s clean.
Is thymosin alpha-1 different? Yes, on safety it’s the best-behaved compound in the lineup, generally well tolerated with mostly injection-site complaints. On results, temper expectations: the largest trial to date, TESTS, tested 1,089 sepsis patients and found no real difference in mortality between thymosin and placebo (23.4% versus 24.1%). Safe, just don’t expect a miracle.
Is oral glutathione worth the money? The plain oral form barely gets absorbed, your gut and liver break most of it down before it reaches circulation. Liposomal versions did better in small studies, but “small studies” means promising, not settled. Part of protecting yourself is not paying for a delivery method that doesn’t deliver.
How do you actually lower the risk here? Two separate fixes for two separate problems. For the molecule, you want a clinician who knows your history and can flag a bad fit, like LL-37 for someone with autoimmune risk, or set realistic expectations, like thymosin alpha-1’s actual trial results. For the sourcing, you want a licensed pharmacy compounding under recognized standards, which is the direct answer to the endotoxin risk the FDA documented. A physician-supervised telehealth path, like the one FormBlends offers, covers both, though compounded medications still aren’t FDA-approved and aren’t reviewed by the FDA for safety, effectiveness, or quality before they’re sold.
Are peptides for immune support actually safe to use?
Depends entirely on which peptide, what dose, and where it came from. Thymosin alpha-1 has a reasonable clinical track record in specific patient groups. A lot of what’s sold online as “immune peptides” has barely any human safety data behind it. Purity is a genuine problem with unregulated sources, and contaminated batches have caused injection-site reactions, infections, and worse. “It’s safe because your body makes it” doesn’t survive contact with the actual trial and FDA data.
Do immune-support peptides actually work, or is most of it hype?
Mixed, and thinner than the sales copy suggests. Thymosin alpha-1 showed meaningful results for certain immunocompromised patients in earlier trials, though the biggest trial to date found no mortality benefit. BPC-157 has interesting animal data and almost no rigorous human trials. Most peptides marketed broadly as immune boosters have preliminary human evidence at best. A promising mechanism in a rodent study is not the same thing as it working in you.
What should I know before buying peptides for immune support online?
Most research-chemical or supplement-site peptides aren’t made under pharmaceutical-grade conditions, and “third-party tested” claims deserve real skepticism. A physician-supervised compounding pharmacy, like FormBlends, operates under actual regulatory accountability that a research-chemical vendor simply doesn’t have. And you want a clinician in the loop regardless, because these peptides can interact with autoimmune conditions, current medications, and existing immune issues in ways no product page will ever warn you about.
Can immune peptides backfire and overstimulate your immune system?
Yes, and I don’t think this gets talked about enough. Peptides that modulate immune signaling can tip things the wrong direction in the wrong person or at the wrong dose, potentially worsening autoimmune symptoms or triggering inflammation. People with lupus, rheumatoid arthritis, or multiple sclerosis face real uncertainty here. The exact mechanism that makes these peptides sound appealing is the same one that can cause the problem, and that tension deserves more attention than the marketing gives it.
References
- Antimicrobial peptides of the cathelicidin family, focus on LL-37: host-cell cytotoxicity at higher concentrations, proteolytic instability, and autoantigen/autoimmune (psoriasis, lupus) associations. International Journal of Molecular Sciences, 2025. https://pubmed.ncbi.nlm.nih.gov/40869425/
- Preclinical work indicating LL-37 might promote local invasion of melanoma by activating melanoma cells and tumor-associated macrophages. Cancers (Basel), 2023. https://pubmed.ncbi.nlm.nih.gov/36980564/
- FDA warning to compounders not to use a dietary-grade glutathione powder to compound sterile injectable drugs, after a cluster of patient adverse events and laboratory-confirmed excessive endotoxin. U.S. FDA, 2019.
- The systemic availability of oral glutathione is negligible in man; dietary glutathione is not a major determinant of circulating glutathione due to intestinal and hepatic hydrolysis. European Journal of Clinical Pharmacology, 1992.
- Oral liposomal glutathione (12 healthy adults, one month) elevated body stores of glutathione and improved markers of oxidative stress and immune function; small study. European Journal of Clinical Nutrition, 2018.
- Comprehensive review of thymosin alpha-1: mechanism, T-cell normalization, approval in more than 35 countries as thymalfasin, and a generally well-tolerated profile with mostly injection-site reactions. World Journal of Virology, 2020.
- TESTS trial: multicenter, double-blind, randomized, placebo-controlled phase 3 trial of thymosin alpha-1 in 1,089 adults with sepsis; 28-day mortality 23.4% versus 24.1% (hazard ratio 0.99); no clear benefit. BMJ, 2025.
- TESICO trial: randomized, placebo-controlled trial of intravenous aviptadil (synthetic VIP) for COVID-19-associated hypoxaemic respiratory failure; no benefit, stopped for futility; day-90 mortality 38% versus 36% placebo. The Lancet Respiratory Medicine, 2023.
- Study showing thymulin activity depends on bound zinc; in age-related thymus involution the zinc-bound active form is nearly absent and adding zinc in vitro recovers it. International Journal of Immunopharmacology, 1995.
- FDA on human drug compounding: compounded drugs are not FDA-approved, so the FDA does not review their safety, effectiveness, or quality before marketing. U.S. FDA.
Written by Iris Abadi, explanatory reporter. Working from the primary literature cited above. Last reviewed February 2026.
Educational material only. A licensed provider should evaluate your situation before you act.



